Submissions to the Hawke’s Bay Hospital Board 1980
[Handwritten]
I support in principle the desirability of an acute complex – not a new hospital between Napier and Hastings – a complex either at Napier or Hastings, however I think that perhaps it will continue as it is – development of both hospitals.
A new hospital is not practical and not viewed favourably by local authorities.
I hope to see the C H Block in Hastings proceed and also planned development in Napier proceed.
{kind=link}
{kind=link}
{kind=link}
HASTINGS CITY COUNCIL
SUBMISSIONS TO THE HAWKE’S BAY HOSPITAL BOARD ON LONG TERM PLANNING OPTIONS
INTRODUCTION
The Hastings City Council feels strongly that a public hospital is an essential element of any complete community. It serves a particularly important service to its community, the preservation or restoration of health and the easing of illness and suffering generally. The public hospital by its very presence gives comfort to the old and confidence to the young. It serves as a focal point for community interest and involvement and is as important to the community as its local government, fire station, police station or post office.
In preparing these submissions Council has tried to be objective and has reached its conclusions on the information available. It is hoped that the Hawke’s Bay Hospital Board will receive them as constructive statements made in a genuine attempt to serve the interests of the whole community.
Inevitably, discussion concerning the placing of public facilities in the Hastings/Napier district, will give rise to claims of parochialism and the long term planning of the hospital service has been no exception. On this occasion, however, the elected community leaders of Hastings and Napier cities are on the same side and claims of parochialism have come more from people either pushing their own personal point of view or serving only extremely narrow interests. We do not believe that the conclusions set down in this document have been reached on parochial grounds nor do we believe that the stance taken by the Napier City Council was adopted on parochial grounds.
Two papers have been circulated, under the name of the Board, outlining the long term planning options as seen by the Board’s officers and these have provided the sole basis for persons and organisations upon which to make decisions on the most appropriate option. While Council commends the Board and its officers for making these papers freely available for comment and also the willingness with which the Board’s officers have made themselves available to speak to interested groups, we feel that the papers are over-simplified and too much vital information is omitted for a really reasoned decision to be reached. Despite these reservations on the papers the Hastings City Council does appreciate the Board’s actions in inviting comment on the planning options and in particular appreciates the opportunity to make submissions to the Board.
The following submissions are composed of four sections dealing with the options in the following manner:
A. Comment on the Hawke’s Bay Hospital Board’s long term planning option papers.
{kind=link}
Page 2
B. Examination of the Hawke’s Bay Hospital service in relation to other hospital services in New Zealand.
C. Planning and social implications of the long term planning options.
D. Summary and conclusions.
Section A
COMMENT ON THE HAWKE’S BAY HOSPITAL BOARD’S LONG TERM PLANNING OPTION PAPERS
Two papers have been circulated by the Hawke’s Bay Hospital Board, one in April and the other in July 1980. Both papers are basically the same with the second one being a more refined and explicit version of the first. The comments which follow may apply to one or both papers.
1. Population
The first paper quoted population figures as under for the year 2001:
Napier City 74,300
Hastings Urban Area 47,600
Total Population 150,000
The figure for the Hastings urban area was in fact incorrect and despite being drawn to the attention of the Board’s officers the paper was further circulated in unaltered form. The inaccuracy aside, we fail to see the reason why individual local authority populations needed to have been mentioned at all. Surely when talking about Hawke’s Bay Hospital Board responsibilities, the total population of the whole of the Board’s district was the only important or relevant figure necessary. However, in respect of Option (1) the only relevant figures are the populations served by the two main hospitals. Even the second paper failed to make the point. In our opinion the papers should both have quoted the total population served by the Board in the Hastings/Napier area and which by the year 2001 will be (on a medium fertility and migration basis) 149,000. In respect of Option (1) (the retaining of two acute hospitals) the populations served by the two hospitals should have been quoted as under:
Hastings Hospital – by the year 2001 77,000
Napier Hospital – by the year 2001 72,000
These figures are on the basis that both hospitals operate as fully commissioned acute hospitals.

{kind=link}
Page 3
2. The Economy
While it is true that the present government has placed emphasis on the New Zealand Planning Council’s recommendation that health funding should be limited to a percentage of gross domestic product there is no guarantee that this will be the case with future governments, even of the National variety. Economic situations can change rapidly and long term decisions should not be made on short term situations.
3. Technology
It is true that technology in all fields of endeavour is changing rapidly and the medical field is no exception. Hand in hand with the advance of medical technology is the advance of communications and it is not only conceivable but almost certain that before long the development of communications will enable the resources of the most advanced data systems, diagnostic services and laboratory facilities to be available to the smallest of hospitals. These developments will assist hospital authorities to maintain treatment centres closer to where people reside.
4. Bed Requirements
Council is not prepared to pass comment on the bed requirements set out in the two papers and considers this largely a matter for the Board to decide. It is worth commenting that on average throughout New Zealand there exists one hospital bed for each 113 persons. In Hawke’s Bay there is only one bed for each 156 persons, one of the highest ratios in the country. It appears, therefore, that the Board’s estimate of additional beds is reasonably accurate. However, with wards closed at the moment, it does not seem to be critical at this stage to decide finally where these beds should be provided. Council is of the opinion that a greater degree of flexibility and economy would result if the additional beds were to be provided as extensions to the existing hospitals in Hastings, Napier and Wairoa.
5. i. Options Generally
The first paper circulated by the Board on page 4 states that the situation regarding hospitals is unusual in Hawke’s Bay in that two major general (acute?) hospitals exist fourteen miles apart and that this situation is unequalled anywhere in New Zealand. Commenting on this statement we would say that to prepare these submissions extensive study was made of the National Health Statistics Centre Hospital Management Data report for 1979. Apart from useful data utilised in Section (B) of these submissions, the strong impression was gained that hospital services throughout New Zealand are largely tailored to meet the needs of the community they serve. It is worth noting that some hospital boards administer up to six general hospitals or up to 23 hospitals of all types. Throughout New Zealand on

{kind=link}
Page 4
average, there is a hospital of some type for every 17,800 persons. In Hawke’s Bay there is one hospital for every 40,900 persons, a figure which is equalled by only one other board district and that is Wellington. Hawke’s Bay may be unique in its hospital services but then that could be said of most areas of New Zealand.
ii. Option 1
In examining Option 1, we would question whether or not this is in fact a single option as it appears to us that it can have three variations. The first which we will call Option l(a) is as outlined in the second paper circulated by the Board. However, it is recalled that some five years ago a major psychopaedic unit was planned for the “cornfield” site in Hastings. Somewhere along the way this unit seems to have been redesignated to the newly purchased Park Island site. As variations to Option 1, we would see Option 1(b) as locating the psychopaedic, younger disabled, geriatric A & R development on fully serviced land owned by the Board in Omahu Road, Hastings. As Option l(c), we see both Napier and Hastings hospitals developed to provide a further 60 beds each to meet the psychopaedic, younger disabled and geriatric A & R requirements in their own districts.
In its present form the Option outlined in the second paper is not acceptable to the Hastings community, nor will it best serve its needs. The Hastings City Council reserves the right to take up the matter of the variations to Option 1 if this is the option finally accepted by the Board for long term purposes.
iii. Option 2
The Board’s officers have obviously seen the major variation to the option and presented it with two alternatives. This is the option which has been what can only be described as the subject of a “hard sell” to various groups and organisations in Hawke’s Bay. Too much information is lacking and too many questions are unanswered for a rational decision to be made on Option 2.
Information needed or questions to be answered include the following:
a. Where could a central site be found to serve both the Napier and Hastings urban areas satisfactorily and yet make efficient use of already provided services such as water supply, sewerage, roading and electricity?
b. Where could a central site be found which could be safe from flooding or which would not run the risk of becoming isolated from the major urban areas in

{kind=link}
Page 5
the event of bad flooding or major earthquake? In the case of disaster a hospital may not only help the community, it may also need the assistance of the community.
c. What would happen to the redundant hospital if Option 2(b) is adopted? Each existing hospital has a Government valuation of about $10 million but would cost several times this amount to replace.
d. What would happen to the claimed economies of a central acute hospital if Option 2(a) were to be adopted? If, as it is claimed, it is inefficient to operate two hospitals within 14 miles of each other, how much more inefficient would it be to operate three hospitals?
e. In the event of Option 2(b) being adopted, one or other of the two major centres would be without a major hospital at all. Would the Board consider that this situation would be reasonable let alone tolerated?
f. In the event of Option 2 being adopted, has the Board obtained from Government any assurance that the money will be forthcoming to complete the central acute hospital within a reasonable time? Further, if the money is forthcoming, how can the Board or indeed the Government, justify the extra loan charges and loan repayments necessary to pay for the new hospital when these charges will amount to over double the claimed savings?
The above questions do need full answers before Option 2 in either of its variations is pursued any further.
iv. Option 3
Obviously this option, for many reasons, would not be acceptable to the Hastings community unless the new acute hospital was sited in Hastings. However, that unlikely, although not altogether inappropriate decision, we would confidently expect be strongly opposed by Napier people – with good reason. We in Hastings would certainly object if the reverse situation arises. We agree with the Board’s officers that Option 3 is not a viable alternative to the present structure of hospital service in Hawke’s Bay.
v. Rationalisation of Services
In the opinion of the Hastings City Council, confirmed by public statements to the same effect by the Chairman of the Hospital Board, rationalisation, particularly as it affects the Hastings Memorial Hospital, has gone quite far enough and in fact has already gone too far.

{kind=link}
Page 6
The further rationalisation of services would in effect mean the moving of all acute services to Napier Hospital – in short Option 3 would, as far as Hastings is concerned, become almost a reality. This situation is absolutely against the welfare of Hastings city, Havelock North borough and surrounding districts and is not acceptable.
6. Implications of Options
i. Land Costs
The Hastings City Council does not consider land costs to be a particularly important facet of the Board’s long term planning options. In the case of retaining the two existing hospitals in Hastings and Napier, land is not a problem. There exists in Hastings at least more than sufficient land to cater for necessary developments in Hastings for the next 50 years let alone the next 20 years – this land is also close to excellent water supply, stormwater, sewage disposal, arterial road services and being near the centre of the largest urban population in Hawke’s Bay could not be bettered for the site of hospital services.
His Worship the Mayor of Napier has publicly announced that there exists on the Napier hospital site ample room for further development and given the likely slow growth of the region over the next 20 years this statement can readily be accepted. Therefore, there appears to be very little reason why the Board should even contemplate further land purchases, particularly land which does not already have ready access to city standard services – in fact it is somewhat puzzling why the Park Island site was purchased.
ii. Construction Costs
Option 1 is quoted in the Board’s papers as costing $36.3 million – discounted to present values to $23 million.
Option 2(a) is quoted as costing $48.2 million – discounted to present values to $29.2 million.
Option 2(b) is quoted as costing $53.4 million.
As claimed economies for a central acute hospital are likely to be offset by additional operating expenses caused by the running of three hospitals to service the Hastings/Napier area, it is more realistic to compare Option 1 with Option 2(b).
In comparing the construction costs involved in the three options we obtain the following present day differences:

{kind=link}
Page 7
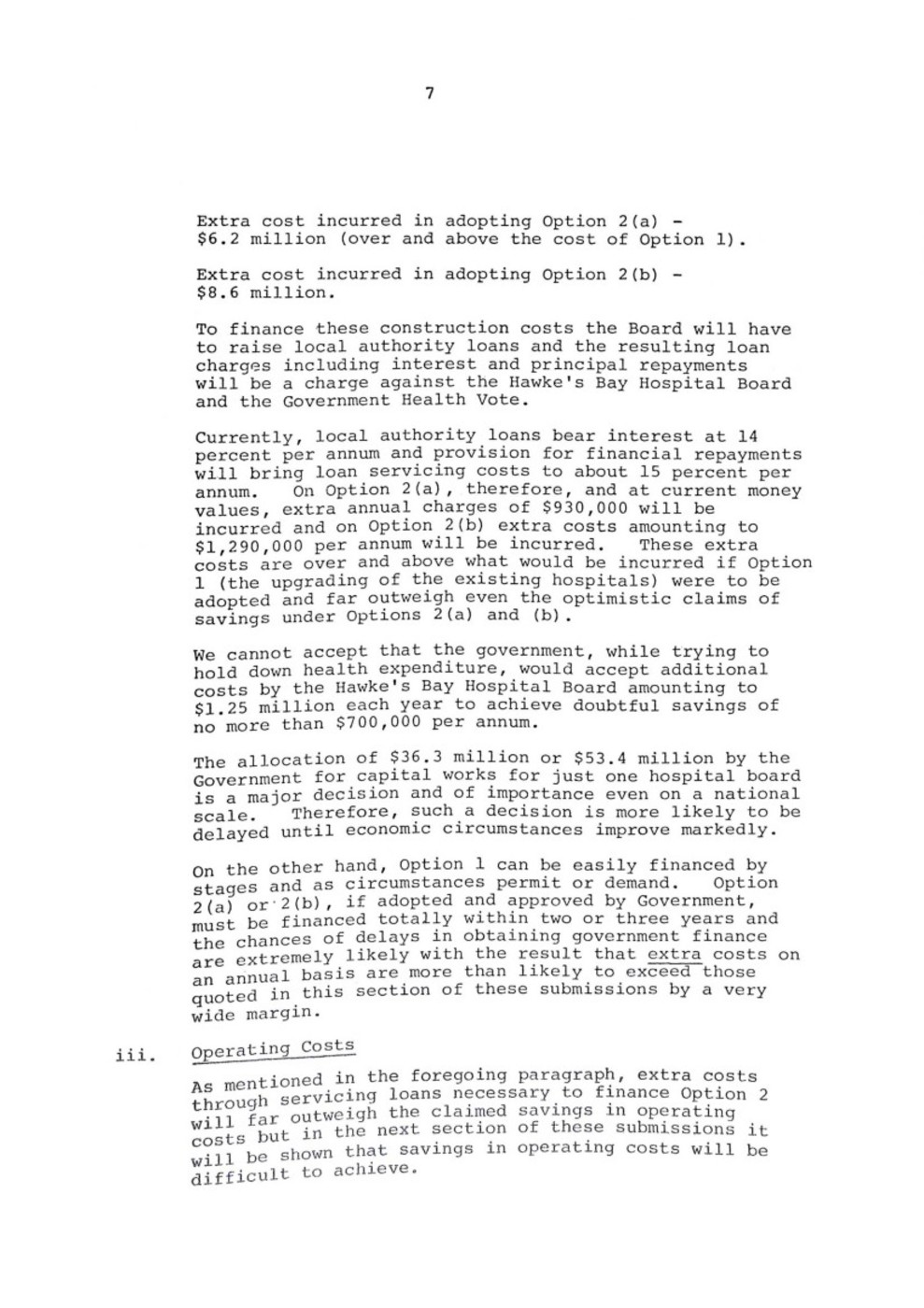
Extra cost incurred in adopting Option 2(a) – $6.2 million (over and above the cost of Option 1).
Extra cost incurred in adopting Option 2(b) – $8.6 million.
To finance these construction costs the Board will have to raise local authority loans and the resulting loan charges including interest and principal repayments will be a charge against the Hawke’s Bay Hospital Board and the Government Health Vote.
Currently, local authority loans bear interest at 14 percent per annum and provision for financial repayments will bring loan servicing costs to about 15 percent per annum. On Option 2(a), therefore, and at current money values, extra annual charges of $930,000 will be incurred and on Option 2(b) extra costs amounting to $1,290,000 per annum will be incurred. These extra costs are over and above what would be incurred if Option 1 (the upgrading of the existing hospitals) were to be adopted and far outweigh even the optimistic claims of savings under Options 2(a) and (b).
We cannot accept that the government, while trying to hold down health expenditure, would accept additional costs by the Hawke’s Bay Hospital Board amounting to $1.25 million each year to achieve doubtful savings of no more than $700,000 per annum.
The allocation of $36.3 million or $53.4 million by the Government for capital works for just one hospital board is a major decision and of importance even on a national scale. Therefore, such a decision is more likely to be delayed until economic circumstances improve markedly.
On the other hand, Option 1 can be easily financed by stages and as circumstances permit or demand. Option 2(a) or 2(b), if adopted and approved by Government, must be financed totally within two or three years and the chances of delays in obtaining government finance are extremely likely with the result that extra costs on an annual basis are more than likely to exceed those quoted in this section of these submissions by a very wide margin.
iii. Operating Costs
As mentioned in the foregoing paragraph, extra costs through servicing loans necessary to finance Option 2 will far outweigh the claimed savings in operating costs but in the next section of these submissions it will be shown that savings in operating costs will be difficult to achieve.

{kind=link}
Page 8
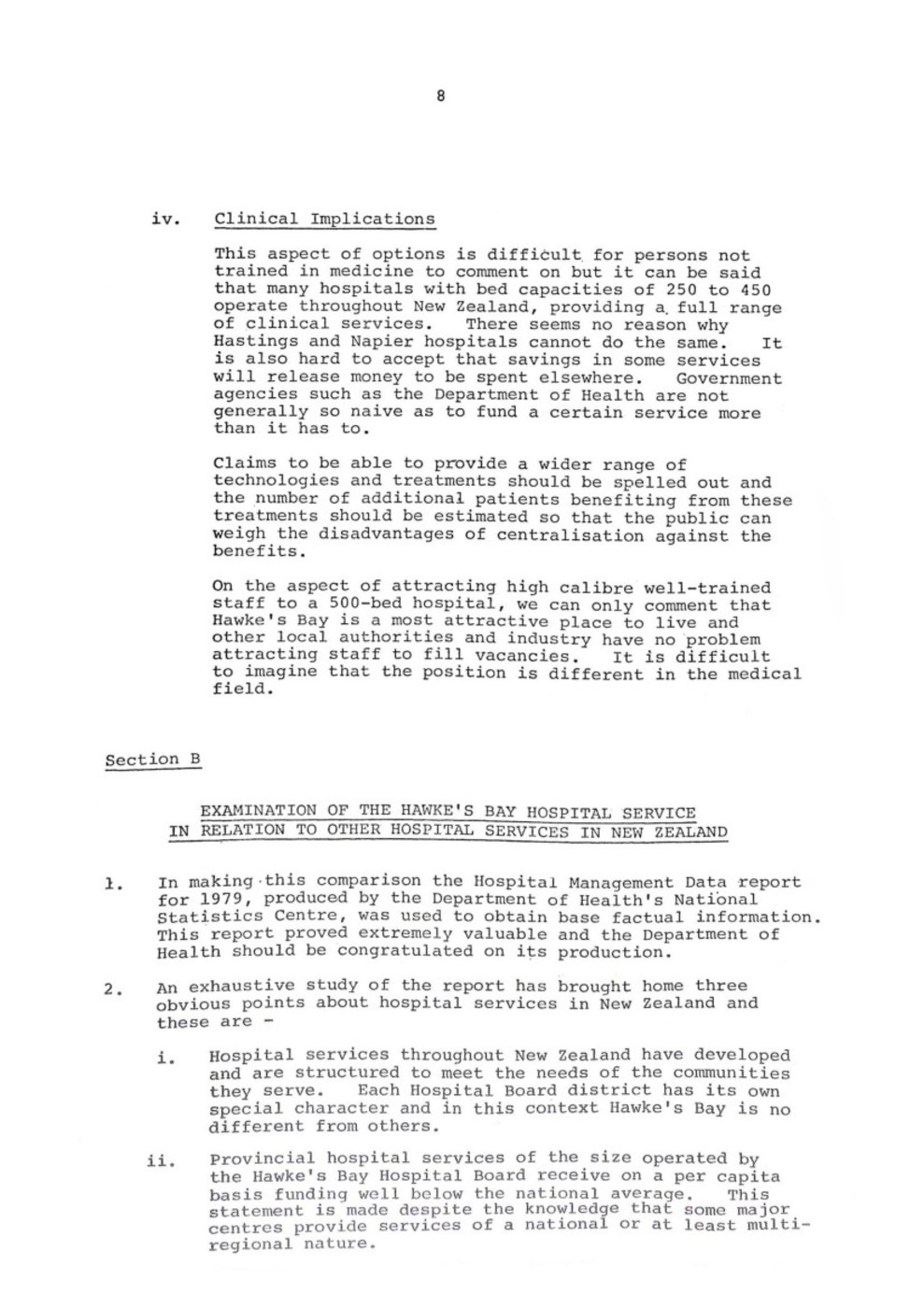
iv. Clinical Implications
This aspect of options is difficult for persons not trained in medicine to comment on but it can be said that many hospitals with bed capacities of 250 to 450 operate throughout New Zealand, providing a full range of clinical services. There seems no reason why Hastings and Napier hospitals cannot do the same. It is also hard to accept that savings in some services will release money to be spent elsewhere. Government agencies such as the Department of Health are not generally so naive as to fund a certain service more than it has to.
Claims to be able to provide a wider range of technologies and treatments should be spelled out and the number of additional patients benefiting from these treatments should be estimated so that the public can weigh the disadvantages of centralisation against the benefits.
On the aspect of attracting high calibre well-trained staff to a 500-bed hospital, we can only comment that Hawke’s Bay is a most attractive place to live and other local authorities and industry have no problem attracting staff to fill vacancies. It is difficult to imagine that the position is different in the medical field.
Section B
EXAMINATION OF THE HAWKE’S BAY HOSPITAL SERVICE IN RELATION TO OTHER HOSPITAL SERVICES IN NEW ZEALAND
1. In making this comparison the Hospital Management Data report for 1979, produced by the Department of Health’s National Statistics Centre, was used to obtain base factual information. This report proved extremely valuable and the Department of Health should be congratulated on its production.
2. An exhaustive study of the report has brought home three obvious points about hospital services in New Zealand and these are –
i. Hospital services throughout New Zealand have developed and are structured to meet the needs of the communities they serve. Each Hospital Board district has its own special character and in this context Hawke’s Bay is no different from others.
ii. Provincial hospital services of the size operated by the Hawke’s Bay Hospital Board receive on a per capita basis funding well below the national average. This statement is made despite the knowledge that some major centres provide services of a national or at least multi-regional nature.

{kind=link}
Page 9
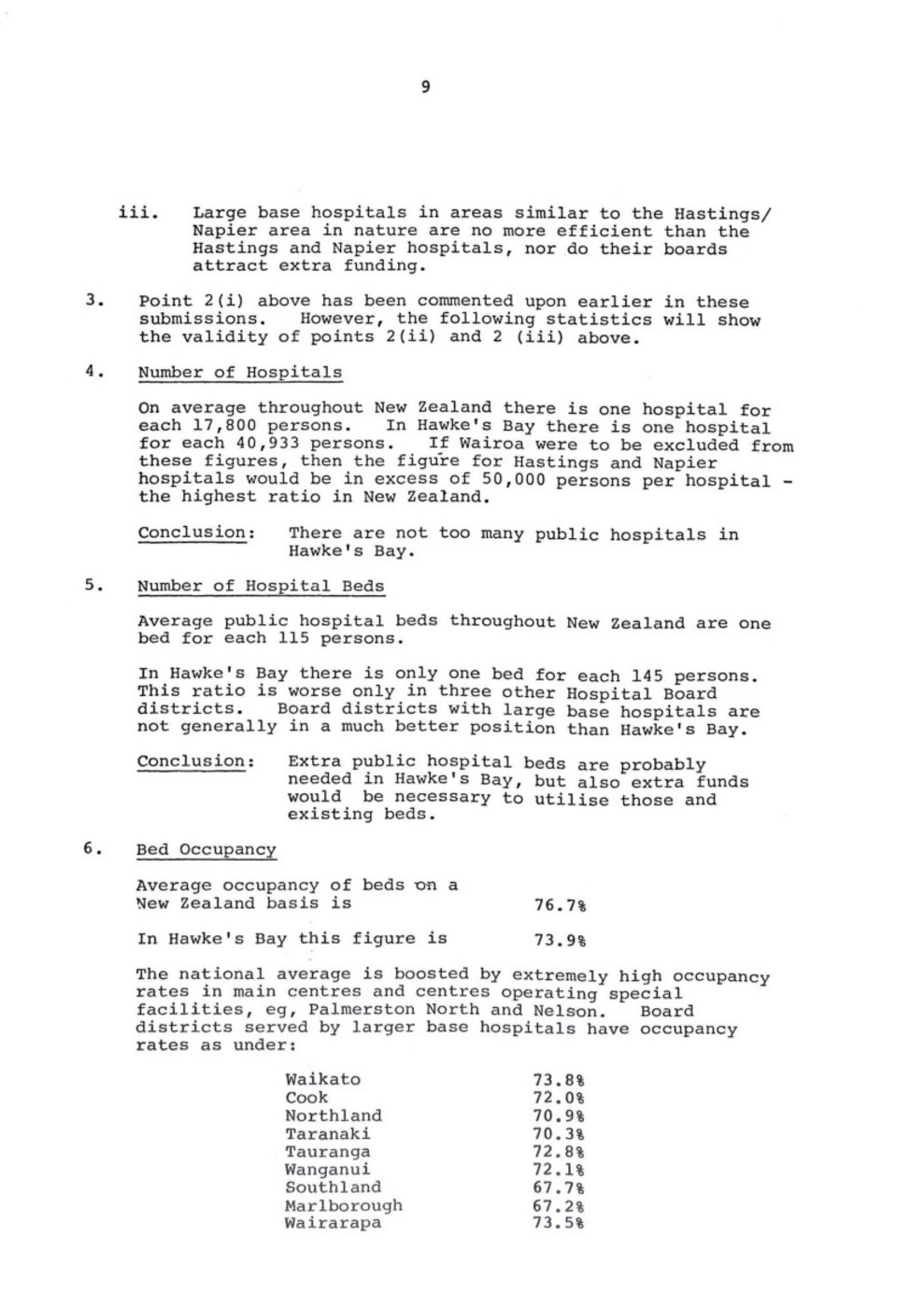
iii. Large base hospitals in areas similar to the Hastings/Napier area in nature are no more efficient than the Hastings and Napier hospitals, nor do their boards attract extra funding.
3. Point 2(i) above has been commented upon earlier in these submissions, However, the following statistics will show the validity of points 2(ii) and 2 (iii) above.
4. Number of Hospitals
On average throughout New Zealand there is one hospital for each 17,800 persons. In Hawke’s Bay there is one hospital for each 40,933 persons. If Wairoa were to be excluded from these figures, then the figure for Hastings and Napier hospitals would be in excess of 50,000 persons per hospital – the highest ratio in New Zealand.
Conclusion: There are not too many public hospitals in Hawke’s Bay.
5. Number of Hospital Beds
Average public hospital beds throughout New Zealand are one bed for each 115 persons.
In Hawke’s Bay there is only one bed for each 145 persons. This ratio is worse only in three other Hospital Board districts. Board districts with large base hospitals are not generally in a much better position than Hawke’s Bay.
Conclusion: Extra public hospital beds are probably needed in Hawke’s Bay, but also extra funds would be necessary to utilise those and existing beds.
6. Bed Occupancy
Average occupancy of beds on a New Zealand basis is 76.7%
In Hawke’s Bay this figure is 73.9%
The national average is boosted by extremely high occupancy rates in main centres and centres operating special facilities, eg, Palmerston North and Nelson. Board districts served by larger base hospitals have occupancy rates as under:
Waikato 73.8%
Cook 72.0%
Northland 70.9%
Taranaki 70.3%
Tauranga 72.8%
Wanganui 72.1%
Southland 67.7%
Marlborough 67.2%
Wairarapa 73.5%

{kind=link}
Page 10
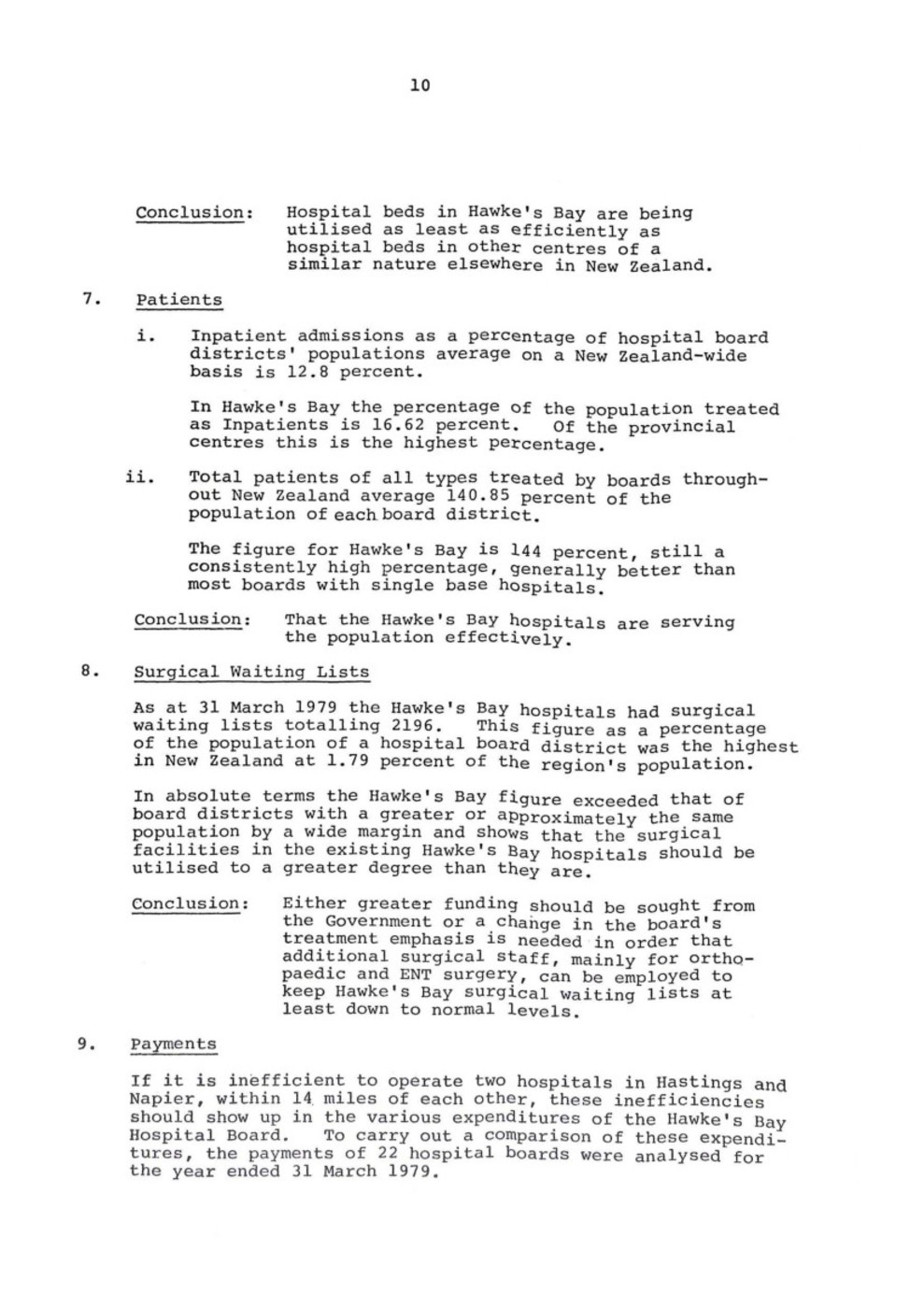
Conclusion: Hospital beds in Hawke’s Bay are being utilised as least as efficiently as hospital beds in other centres of a similar nature elsewhere in New Zealand.
7. Patients
i. Inpatient admissions as a percentage of hospital board districts’ populations average on a New Zealand-wide basis is 12.8 percent.
In Hawke’s Bay the percentage of the population treated as Inpatients is 16.62 percent. Of the provincial centres this is the highest percentage.
ii. Total patients of all types treated by boards throughout New Zealand average 140.85 percent of the population of each board district.
The figure for Hawke’s Bay is 144 percent, still a consistently high percentage, generally better than most boards with single base hospitals.
Conclusion: That the Hawke’s Bay hospitals are serving the population effectively.
8. Surgical Waiting Lists
As at 31 March 1979 the Hawke’s Bay hospitals had surgical waiting lists totalling 2196. This figure as a percentage of the population of a hospital board district was the highest in New Zealand at 1.79 percent of the region’s population.
In absolute terms the Hawke’s Bay figure exceeded that of board districts with a greater or approximately the same population by a wide margin and shows that the surgical facilities in the existing Hawke’s Bay hospitals should be utilised to a greater degree than they are.
Conclusion: Either greater funding should be sought from the Government or a change in the board’s treatment emphasis is needed in order that additional surgical staff, mainly for orthopaedic and ENT surgery, can be employed to keep Hawke’s Bay surgical waiting lists at least down to normal levels.
9. Payments
If it is inefficient to operate two hospitals in Hastings and Napier, within 14 miles of each other, these inefficiencies should show up in the various expenditures of the Hawke’s Bay Hospital Board. To carry out a comparison of these expenditures, the payments of 22 hospital boards were analysed for the year ended 31 March 1979.

{kind=link}
Page 11
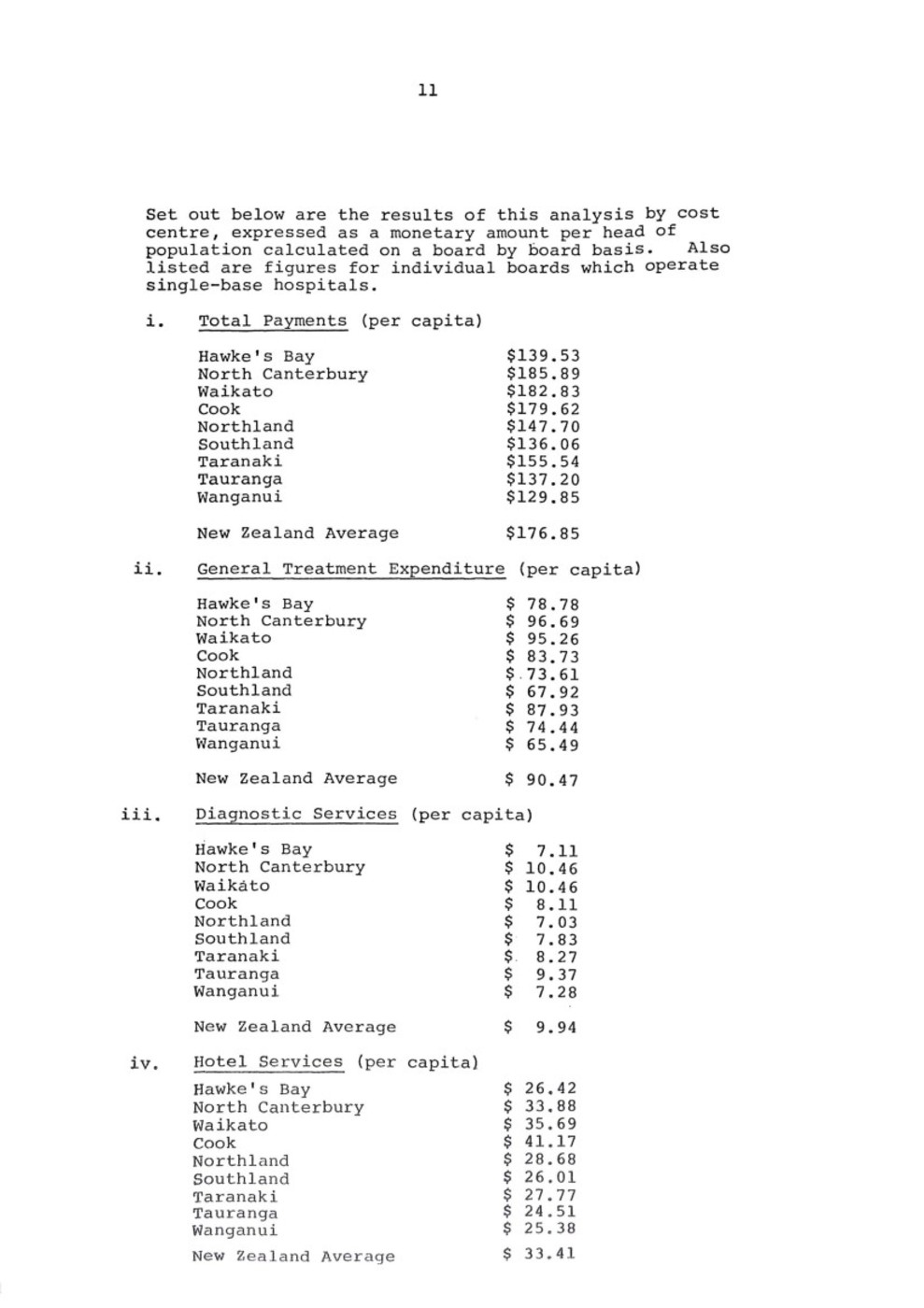
Set out below are the results of this analysis by cost centre, expressed as a monetary amount per head of population calculated on a board by board basis. Also listed are figures for individual boards which operate single-base hospitals.
i. Total Payments (per capita)
Hawke’s Bay $139.53
North Canterbury $185.89
Waikato $182.83
Cook $179.62
Northland $147.70
Southland $136.06
Taranaki $155.54
Tauranga $137.20
Wanganui $129.85
New Zealand Average $176.85
ii. General Treatment Expenditure (per capita)
Hawke’s Bay $78.78
North Canterbury $96.69
Waikato $95.26
Cook $83.73
Northland $73.61
Southland $67.92
Taranaki $87.93
Tauranga $74.44
Wanganui $65.49
New Zealand Average $90.47
iii. Diagnostic Services (per capita)
Hawke’s Bay $7.11
North Canterbury $10.46
Waikato $10.46
Cook $8.11
Northland $7.03
Southland $7.83
Taranaki $8.27
Tauranga $9.37
Wanganui $7.28
New Zealand Average $9.94
iv. Hotel Services (per capita)
Hawke’s Bay $26.42
North Canterbury $33.88
Waikato $35.69
Cook $41.17
Northland $28.68
Southland $26.01
Taranaki $27.77
Tauranga $24.51
Wanganui $25.38
New Zealand Average $33.41

{kind=link}
Page 12
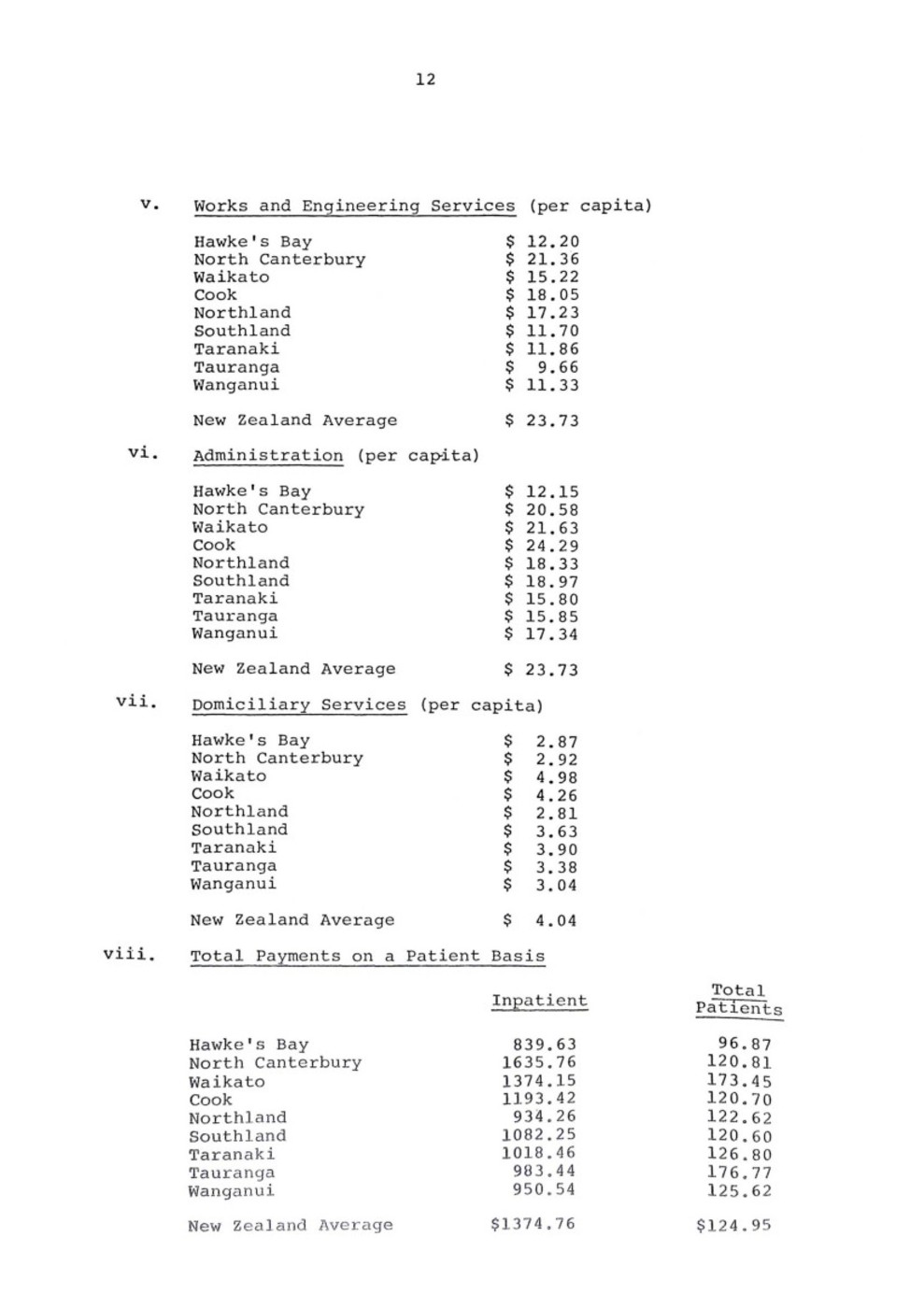
v. Works and Engineering Services (per capita)
Hawke’s Bay $12.20
North Canterbury $21.36
Waikato $15.22
Cook $18.05
Northland $17.23
Southland $11.70
Taranaki $11.86
Tauranga $9.66
Wanganui $11,33
New Zealand Average $23.73
vi. Administration (per capita)
Hawke’s Bay $12.15
North Canterbury $20.58
Waikato $21.63
Cook $24.29
Northland $18.33
Southland $18.97
Taranaki $15.80
Tauranga $15.85
Wanganui $17.34
New Zealand Average $23.73
vii. Domiciliary Services (per capita)
Hawke’s Bay $2.87
North Canterbury $2.92
Waikato $4.98
Cook $4.26
Northland $2.81
Southland $3.63
Taranaki $3.90
Tauranga $3.38
Wanganui $3.04
New Zealand Average $4.04
viii. Total Payments on a Patient Basis
Inpatient Total Patients
Hawke’s Bay 839.63 96.87
North Canterbury 1635.76 120.81
Waikato 1374.15 173.45
Cook 1193.42 120.70
Northland 934.26 122.62
Southland 1082.25 120.60
Taranaki 1018.46 126.80
Tauranga 983.44 176.77
Wanganui 950.54 125.62
New Zealand Average $1374.76 $124.95

{kind=link}
Page 13
Conclusions:
a. That the Hawke’s Bay Hospital Board is shown to be under-funded by the Government and the Hawke’s Bay community is not getting its fair share of the national health vote and this conclusion applies to other provincial centres as well.
b. With low expenditure on all cost centres, despite a high throughput of patients, it cannot be said that the existing hospital structure in Hawke’s Bay is inefficient or in need of restructuring in any way.
c. Any extra funding available from Government would be better utilised in employing extra staff to improve patient treatment rather than the construction of a new central hospital.
Section C
PLANNING AND SOCIAL IMPLICATIONS
From a planning point of view the Hastings City Council, in common with the Napier City Council and Hawke’s Bay County Council, sees major problems in siting a new major hospital in a site central to both Hastings and Napier.
Finding a site between the two cities, which has ready access to major services such as sewerage disposal facilities, road access, water supply and a stormwater system would be almost impossible. Much of the land between the cities is flood plain and although the Hawke’s Bay Catchment Board provides reasonable flood protection, the possibility that the area could not be affected seriously by flooding cannot be taken for granted.
The practicalities associated with setting up a major institution such as a 500-bed hospital in a purely rural area are fearsome. Large amounts of expenditure would be involved which would not be otherwise incurred, probably much of it falling on one or more local authorities. Although these costs may not fall directly on the Board they are nevertheless a cost on the community.
Apart from the provision of basic services by a single central acute hospital, an improvement in the standard of public transport would be needed to give access to the hospital by visitors, day-patients and out-patients, not all of whom have private transport.
The likely isolation of the major hospital from either or both cities will no doubt result in less support from voluntary organisations and less involvement with hospital affairs by both organisations and individuals. The Board’s papers state that

{kind=link}
Page 14
this involvement is likely to reduce anyway – so perhaps the Board’s officers see this as desirable. We do not, and less involvement in the hospitals by voluntary workers will in the end mean greater expenditure on replacement services.
From a social point of view there is only one option and that is Option l. Both Option 2(a), 2(b) and 3 mean effectively that both Hastings and Napier cities will lose either completely or partially their own hospitals and the repercussions could be quite serious for both communities.
Section D
SUMMARY AND CONCLUSIONS
From the foregoing submissions it can be concluded that to remove acute hospital services from either Hastings or Napier would be a retrograde step for hospital services in both communities.
If Option 2 is adopted in either of its variations substantial extra costs will be incurred by both the Hawke’s Bay Hospital Board and the Hawke’s Bay community.
Against the claimed savings of $700,000 for a central acute hospital (and these savings have in fact almost no chance of being realised) are the following costs:
– Community Cost (transport etc) $300,000 p.a.
– Staff Travelling Expenses (estimated) $300,000 p.a.
– Extra Loan Charges (over and above Option 1)
Option 2(a) $930,000 p.a,
or Option 2 (b) $1,290,000 p.a.
This means that the Government and community will be asked to pay at least $1 million per year more for a central acute hospital than for an upgrading of the existing hospital for no real increase in the level of treatment.
National statistics show quite clearly that no real increase in the overall level of treatment can be expected from a single acute hospital and any likely increase is likely to be small and of benefit to only a limited number of patients. Currently in Hastings anyway, casualty cases and outpatients are treated reasonably quickly and any person who has had the frustrating experience of these departments in major centres will certainly realise our present hospital is much to be preferred.

{kind=link}
Page 15
Figures listed in Section B show that while the Hawke’s Bay Hospitals are obviously under-funded by Government they would not be significantly better off with a single acute hospital – in fact the reverse may well be the case. The Hawke’s Bay Hospital Board and its management team is to be congratulated on running three hospitals on its current level of funding and we are sure that all local authorities in the Board’s district would gladly join with the Board in approaching Government for a higher level of funding to help restore services and reduce surgical waiting lists.
Finally, Hastings City Council would respectfully wish to draw attention to the following conclusions:
a. The building of a new central acute hospital is unnecessary and although some indeterminate operating costs may be saved, such a hospital will involve the Board in heavy extra financial annual charges in respect of loans and the community and board staff in heavy and unnecessary extra costs of transport and travelling time.
b. The existing Hastings and Napier hospitals provide a good service to their communities from their existing sites and both should be developed progressively to meet the requirements of their communities.
c. Further rationalisation of services between the Hastings and Napier hospitals should not be contemplated and strenuous attempts should be made to restore full facilities to Hastings Hospital.
d. The planning problems and engineering practicalities associated with building a central acute hospital between Hastings and Napier will inevitably mean delays in improving the medical services in Hawke’s Bay. While Option 2 has the support, even in principle, of the Board it is likely that the Government will delay approvals for upgrading of facilities in Hastings and Napier hospitals with the result that the level of treatment and accommodation in the area may be seriously prejudiced.
e. The Hastings City Council requests that the Hawke’s Bay Hospital Board abandon the suggestion of building a new central acute hospital and the closing or partial closing of either or both the existing Hastings and Napier hospitals and suggests that the Board pursue Option 1 only.
f. The Hastings City Council offers its assistance and co-operation to the Hawke’s Bay Hospital Board in any representations to Government to obtain a higher level of funding for the Board’s hospital services.
HASTINGS
24 September 1980
A.E. Baker
CHIEF EXECUTIVE OFFICER AND TOWN CLERK

{kind=link}
Original digital file
BallantyneDA620_HospitalBoard-1.pdf
Non-commercial use

This work is licensed under a Attribution-NonCommercial 3.0 New Zealand (CC BY-NC 3.0 NZ).
Commercial Use
Please contact us for information about using this material commercially.Can you help?
The Hawke's Bay Knowledge Bank relies on donations to make this material available. Please consider making a donation towards preserving our local history.
Visit our donations page for more information.
Business / Organisation
Hastings City CouncilFormat of the original
Paper documentDate published
24 September 1980Accession number
501776Supporters and sponsors
We sincerely thank the following businesses and organisations for their support.




Do you know something about this record?
Please note we cannot verify the accuracy of any information posted by the community.